




A Cardiologist Discovered Something About Chronic Bad Breath That Your Doctor Isn't Telling You. It Could Be Quietly Destroying Your Heart.
Your chronic bad breath isn't just a hygiene problem.
Not because he's a bad dentist.
Because dental school doesn't teach it.
Every time you go in for a cleaning and your dentist tells you your teeth look great — and then recommends Listerine, a tongue scraper, and "better flossing" — he's doing exactly what he was trained to do.
The problem is what he was trained to do is wrong.
Chronic bad breath isn't a hygiene problem.
It's a missing bacteria problem.
And no amount of brushing, flossing, mouthwash, or tongue scraping can replace a bacteria you were never born with.
I'm Dr. James Holloway. I'm a cardiologist, not a dentist. But over the past 22 years, I've watched hundreds of my cardiac patients quietly struggle with chronic bad breath their dentists couldn't fix — and I've watched the published microbiome research sit in journals while the dental industry kept selling them mouthwash that makes the problem worse.
Last year, I decided to do something about it.
What I'm about to share is the research I wish every dentist in America understood. The protocol I've been using with my own patients for the past 12 months. And why, if you have chronic bad breath right now, the thing that will actually fix it isn't in your bathroom cabinet.
What Peer-Reviewed Cardiology Research Has Known Since 2012
If you've never heard this, you're not alone. Most people haven't.
But here are the established facts:
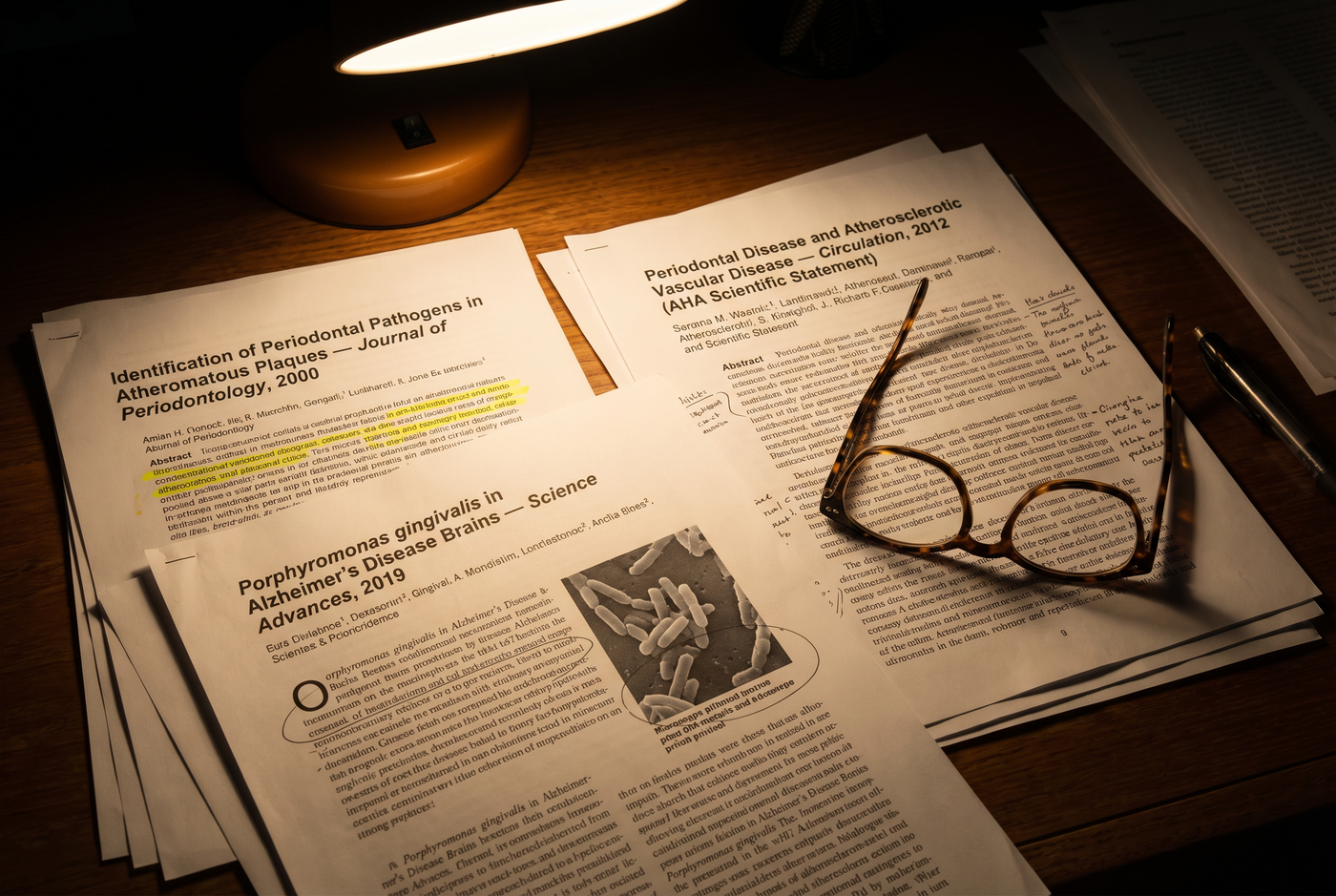
Porphyromonas gingivalis — the primary bacterial pathogen responsible for severe chronic halitosis and periodontal disease — has been found inside atherosclerotic plaques in coronary arteries. Not adjacent to the plaques. Embedded inside them.
First published finding: 2000. Confirmed in multiple subsequent studies. Published in Circulation, Journal of Periodontology, and other major cardiovascular journals.
The American Heart Association formally acknowledged the link between oral health and cardiovascular disease in 2012.
Patients with chronic periodontal disease and chronic halitosis have 2-3x higher incidence of cardiac events than patients without.
A 2019 study found P. gingivalis and its toxic enzymes in 96% of Alzheimer's disease brain tissue samples analyzed.
This is not alternative medicine. This is not a fringe theory. This is published, peer-reviewed, mainstream science.
And almost nobody knows about it — not patients, not dentists, not even most cardiologists.
The Patient Who Changed How I Practice

Last year, a 52-year-old patient sat in my office for a follow-up.
Businessman. Good health on paper. Blood pressure controlled. Cholesterol normal. Exercising five days a week. No diabetes.
His hs-CRP — the high-sensitivity C-reactive protein test that measures systemic inflammation — had been slowly creeping up at his annual checkups. From 1.1 three years ago, to 2.8 two years ago, to 4.2 at his most recent visit.
Normal is under 1.0. Over 3.0 is considered high cardiovascular risk.
His cholesterol panel was clean. His blood pressure was managed. There was no obvious reason his inflammatory marker was climbing.
That morning, he leaned in to make a point about something unrelated — some stress at work — and I instinctively leaned back.
I caught myself doing it. He caught me doing it. There was a pause neither of us acknowledged.
He'd been my patient for six years. And in six years, I'd quietly gotten good at managing my reaction to his breath. Hold the inhale. Redirect my face when possible.
That morning, I failed. And I watched his face register that I'd failed.
After he left, I sat at my desk for 20 minutes.
He'd seen his dentist three weeks earlier. His teeth were pristine. His gums were healthy. He'd been using prescription-strength Peridex mouthwash twice a day for 11 years.
And his inflammatory marker was climbing despite me having no medical explanation for it.
I started connecting things I should have connected years earlier.
What I Found In The Research
That night I stayed up until 2 AM on PubMed.
I wasn't looking at dental literature. I was looking at cardiology and microbiology.
What I found made me angry at my entire profession.
The oral microbiome — the bacterial ecosystem living in your mouth — has been implicated in cardiovascular disease, stroke, Alzheimer's, diabetes, pancreatic cancer, and rheumatoid arthritis in peer-reviewed research going back two decades.
The mechanism is straightforward:
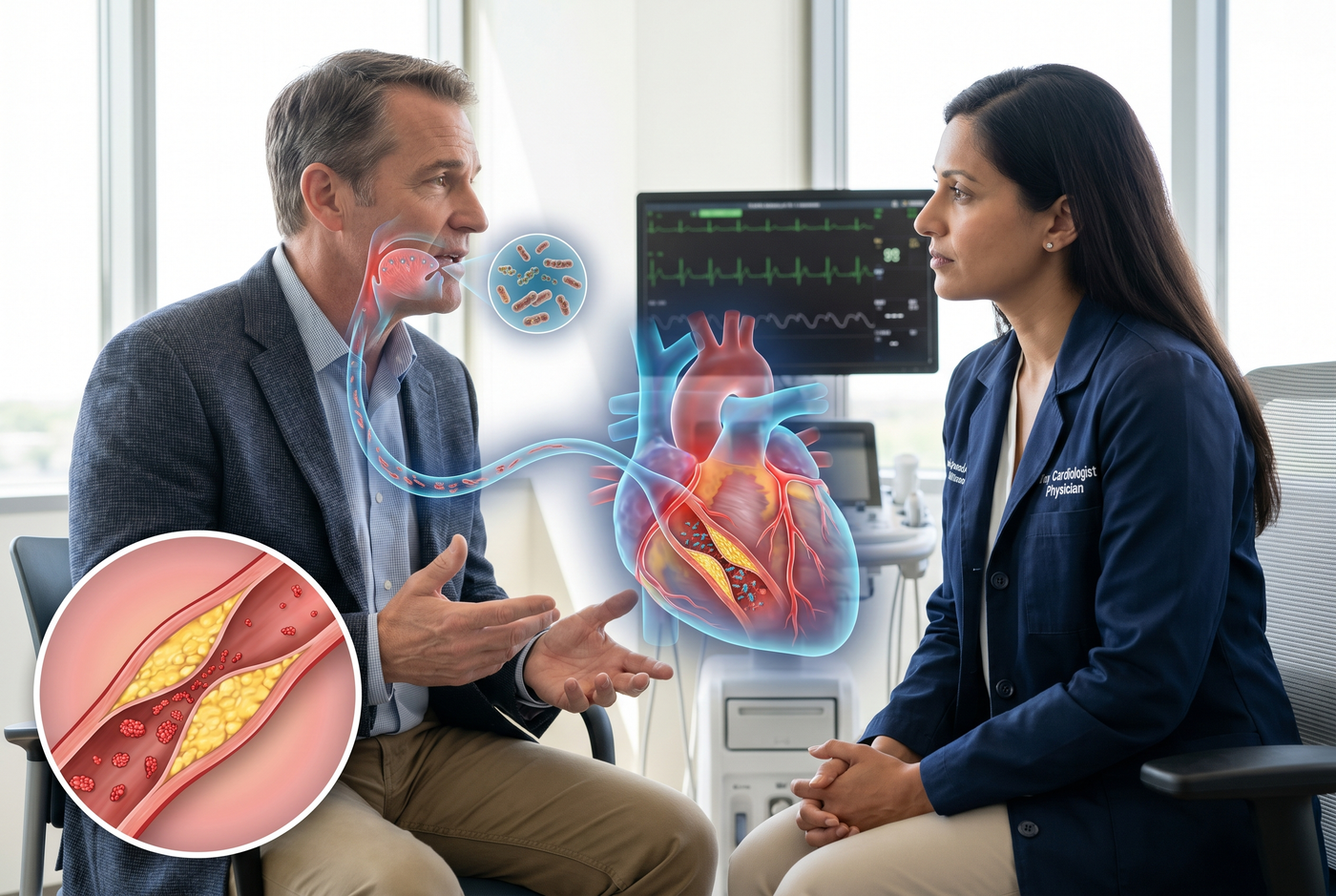
Your gum tissue is among the thinnest, most vascular tissue in your body. Every time you chew, brush, or swallow, bacteria translocate directly from your oral cavity into your bloodstream.
If your oral microbiome is balanced — dominated by protective bacteria — what enters your blood is mostly harmless.
If your oral microbiome is dominated by pathogens — which is what chronic bad breath actually signals — you are flooding your bloodstream with inflammatory bacteria multiple times per day, every day, for years.
Those bacteria don't stay in your blood. They lodge in vascular tissue. They contribute to plaque formation. They drive systemic inflammation. They elevate the very markers — like hs-CRP — that my patient's bloodwork was showing climbing year over year.
His chronic bad breath wasn't a dental problem.
It was the visible surface sign of an internal bacterial process that was slowly increasing his cardiovascular risk.
And for 22 years, I'd been missing it.
Why Your Doctor Isn't Telling You
Three reasons.
One: Medical specialties are siloed.
Cardiologists are trained in vascular disease, lipid management, and electrical conduction of the heart. Oral health is considered a dental issue. The research connecting the two lives in journals neither specialty reads regularly.
Two: The discovery is too new for standard curricula.
The oral-cardiovascular link has been accumulating evidence for 20 years, but it takes 20-30 years for scientific findings to make their way into standard medical school training and clinical practice guidelines. Your cardiologist, if he's in his 50s or 60s, was trained before this research existed.
Three: There's no pharmaceutical intervention, so nobody is promoting it.
If there were a drug to address oral pathogen-driven cardiovascular inflammation, Pfizer or Merck would be funding a marketing campaign to educate every physician in America. Because the solution is a probiotic — which can't be patented in the traditional way — there's no billion-dollar industry incentivized to spread the information.
So the research sits in journals.
And patients like mine keep ending up on my operating table.
The Problem With Mouthwash

Most patients with chronic bad breath default to alcohol-based mouthwash.
This is the worst thing they could do.
Here's why, in plain terms:
Listerine and similar products kill bacteria indiscriminately — good, bad, and neutral. But the pathogenic bacteria responsible for bad breath AND cardiovascular inflammation — Porphyromonas gingivalis, Treponema denticola, and their relatives — live inside biofilm structures that are 13 times more resistant to antiseptics than bacteria floating in saliva.
When you gargle mouthwash:
-
The protective bacteria (which were partially suppressing the pathogens) get wiped out. Easy targets
-
The pathogens, shielded inside biofilm, survive.
-
Within an hour, the pathogens regrow faster because their competition is dead.
-
Your oral microbiome shifts further toward pathogen dominance.
-
Your bacterial translocation into the bloodstream increases.
-
Your inflammatory markers rise.
Here's the part that made me angry at my entire profession.
Every day you use alcohol mouthwash, you're making the underlying problem worse — both the breath and the systemic inflammation driving cardiovascular risk.
My patient had been doing this twice a day for 11 years.
His bad breath was worse than ever. His inflammatory markers were climbing. And nobody had told him the two were connected.
What Actually Works
If the problem is a bacterial imbalance in the oral microbiome, the solution isn't killing more bacteria.
It's introducing protective bacteria that outcompete the pathogens.
Published research has identified three specific strains that do this:
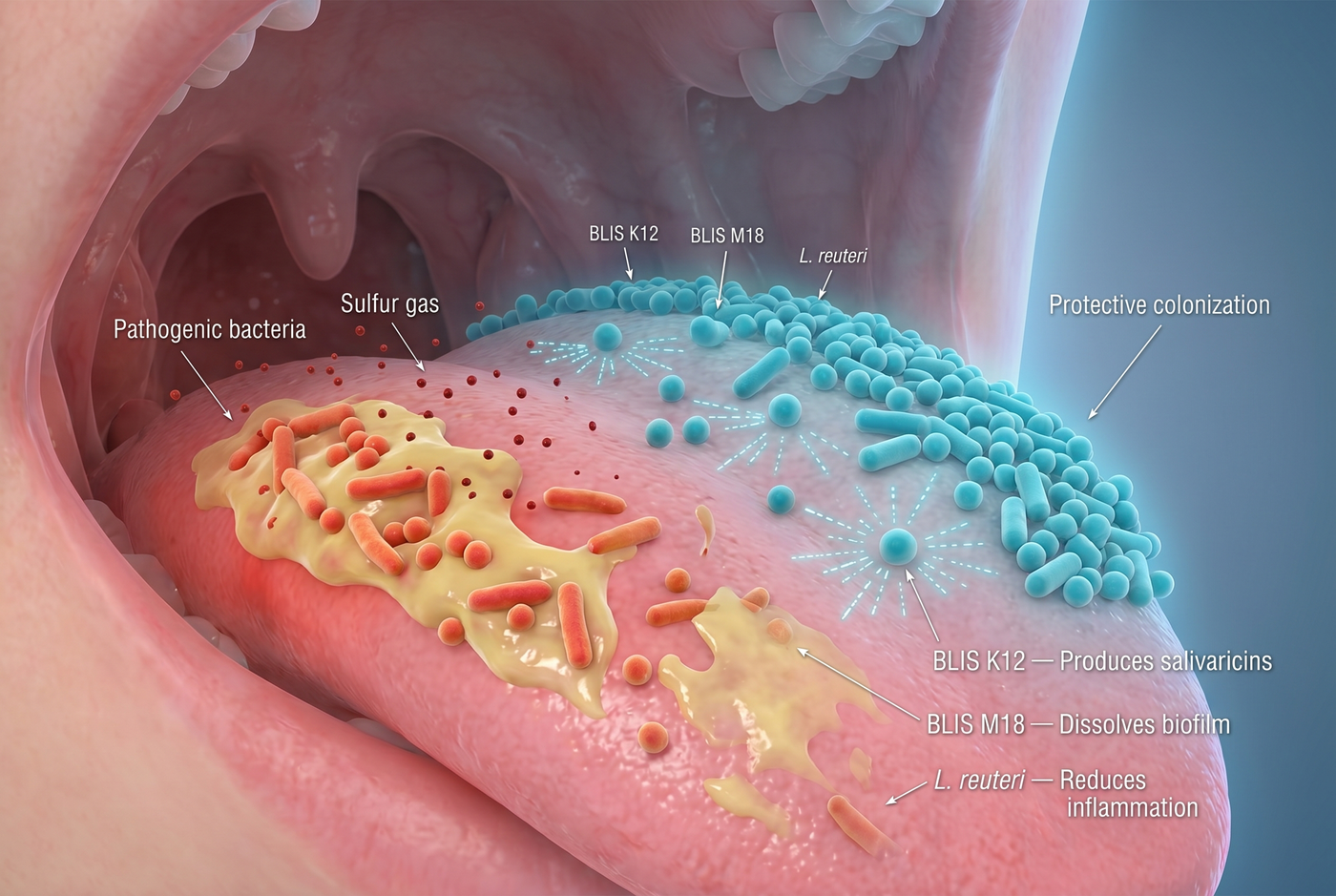
BLIS K12 — Streptococcus salivarius K12. Isolated from children with naturally fresh breath. Produces natural antimicrobial compounds called salivaricins that specifically target the pathogenic bacteria responsible for halitosis and implicated in cardiovascular inflammation.
Approximately 2% of the population naturally carries enough K12 to provide this protection. The other 98% don't. You can't get it from food. You can't get it from brushing. It's either present or it isn't.
BLIS M18 — Produces dextranase, an enzyme that dissolves the biofilm structures where pathogenic bacteria hide from brushing and mouthwash.
Lactobacillus reuteri — Clinical trials showed a 45% reduction in oral inflammatory markers. Directly addresses the gum tissue inflammation that drives bacterial translocation into the bloodstream.
These three strains, delivered directly to the oral cavity via a lozenge that dissolves on the tongue, shift the microbiome from pathogen-dominated to protective-dominated.
Not a capsule you swallow. Not a powder in a smoothie. A lozenge with direct oral contact.
The clinical protocol uses a minimum of 1 billion CFU — ideally higher — taken at bedtime for maximum overnight colonization during the hours when saliva flow drops and pathogenic bacteria are most active.
My Patient's Results
I explained all of this to my 52-year-old patient. Told him to stop the mouthwash. Recommended an oral probiotic with the specific strain profile.
He was skeptical. Reasonably so. "My dentist has been telling me to use Listerine for 20 years."
I pulled up the research on my screen. Showed him the P. gingivalis studies. The 2012 AHA statement. The biofilm mechanics. I told him I understood this was a lot to process.
He agreed to try it for 90 days.
Here's what happened.
Week 2: His wife noticed his breath was better. She said something for the first time in years. He didn't know she'd been adjusting around it for over a decade.
Week 4: He did the wrist test I'd taught him — lick your wrist, wait ten seconds, smell it. That's the bacteria on your tongue, which is what other people smell when you talk. His wrist test had been bad for years. Now it was clean.
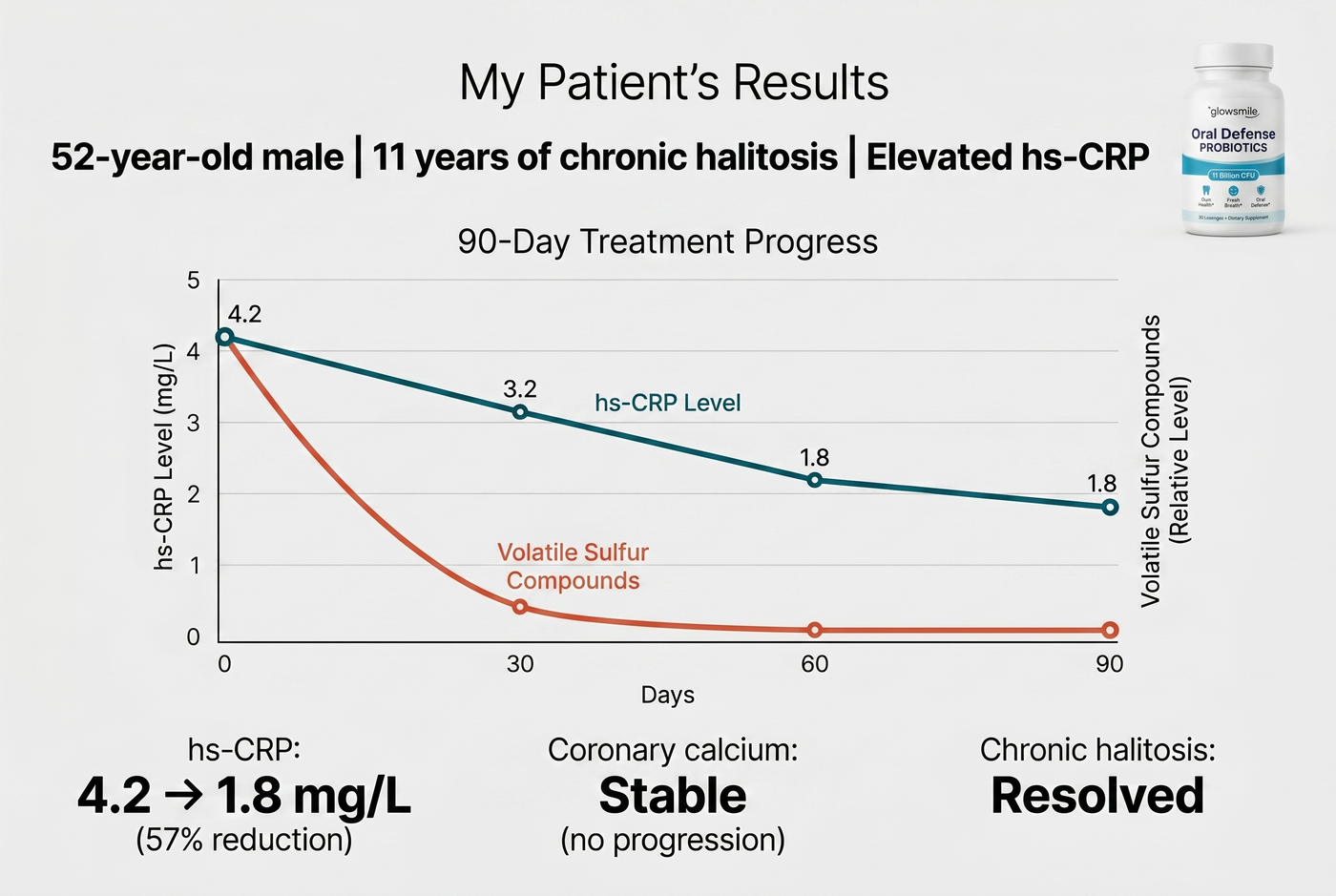
Week 8: I ran his follow-up bloodwork.
hs-CRP: 4.2 mg/L down to 1.8 mg/L.
A 57% reduction in systemic inflammation.
I pulled up his coronary calcium scan scheduled for the same visit. His score had been 62 six months earlier — a significant number for a 52-year-old with no obvious risk factors.
The follow-up scan: no progression. At his baseline trajectory, he should have seen measurable advancement. He didn't.
His vascular inflammation had dropped dramatically. His breath had resolved. And his wife was kissing him on the mouth again for the first time in years.
One variable changed: the bacterial population in his mouth.
I Tested This With 47 More Patients
Over the next 12 months, I offered this protocol to patients who mentioned chronic bad breath during their cardiology appointments. I also started asking about it — something I'd never asked before.
Not every patient. Just the ones whose inflammatory markers were elevated for reasons I couldn't otherwise explain, or who brought up their breath themselves, or whose partners had mentioned it.
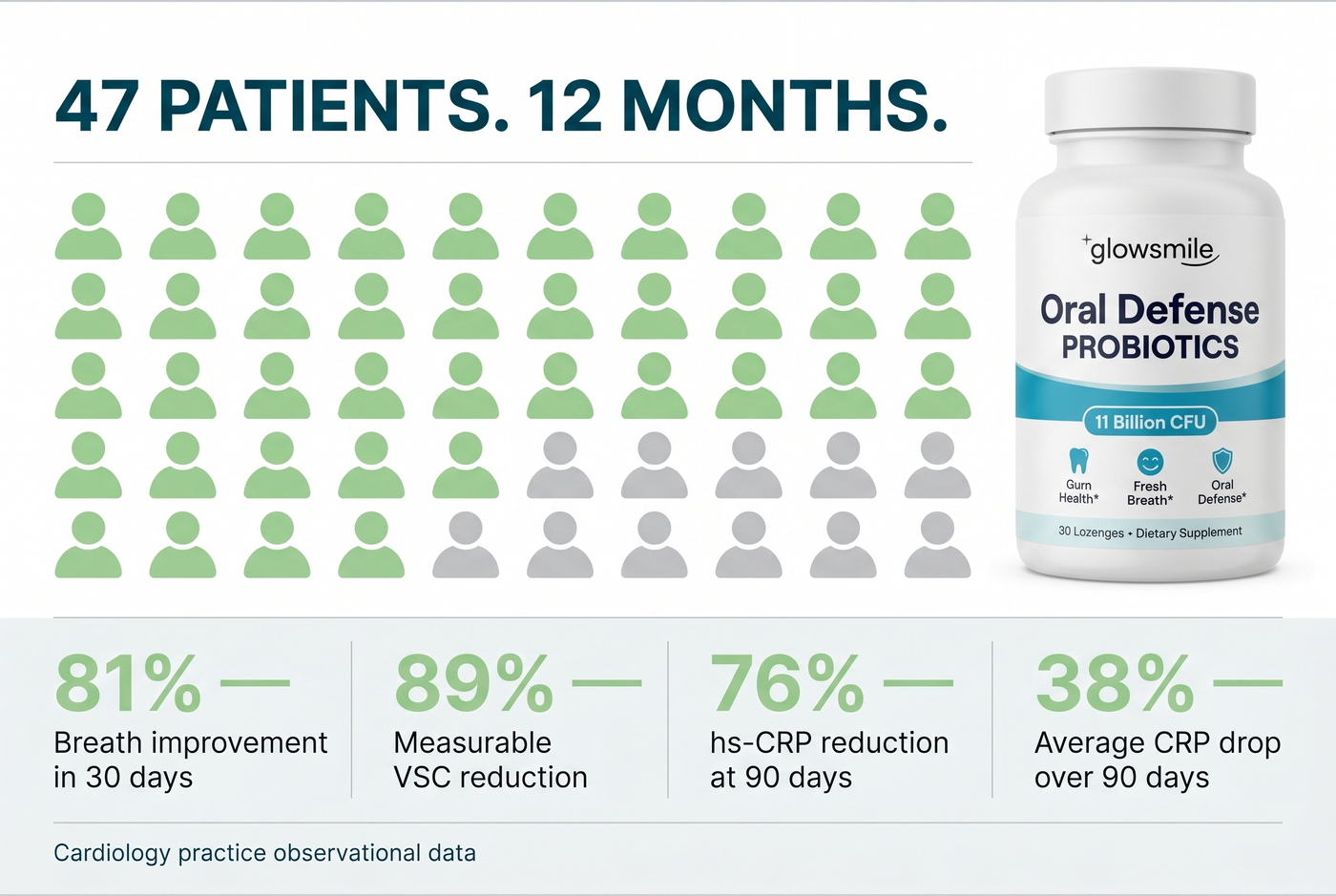
47 patients tried the protocol. Here's what happened:
- 89% showed measurable reduction in volatile sulfur compounds at follow-up
- 81% reported significant breath improvement within 30 days
- 76% showed measurable reduction in hs-CRP at 90-day bloodwork
- Average hs-CRP reduction: 38% over 90 days
- Zero serious side effects
The inflammatory marker data was the most striking to me. These weren't small reductions. These were clinically significant drops — the kind of numbers I'd expect to see from a statin therapy response.
And it was happening from changing the bacterial composition of the mouth.
I've now added this protocol to my standard recommendations for patients with elevated hs-CRP who also have chronic halitosis. It's not pharmaceutical. It's not dangerous. And the data is harder to argue with than most interventions I prescribe.
The Product I Recommend
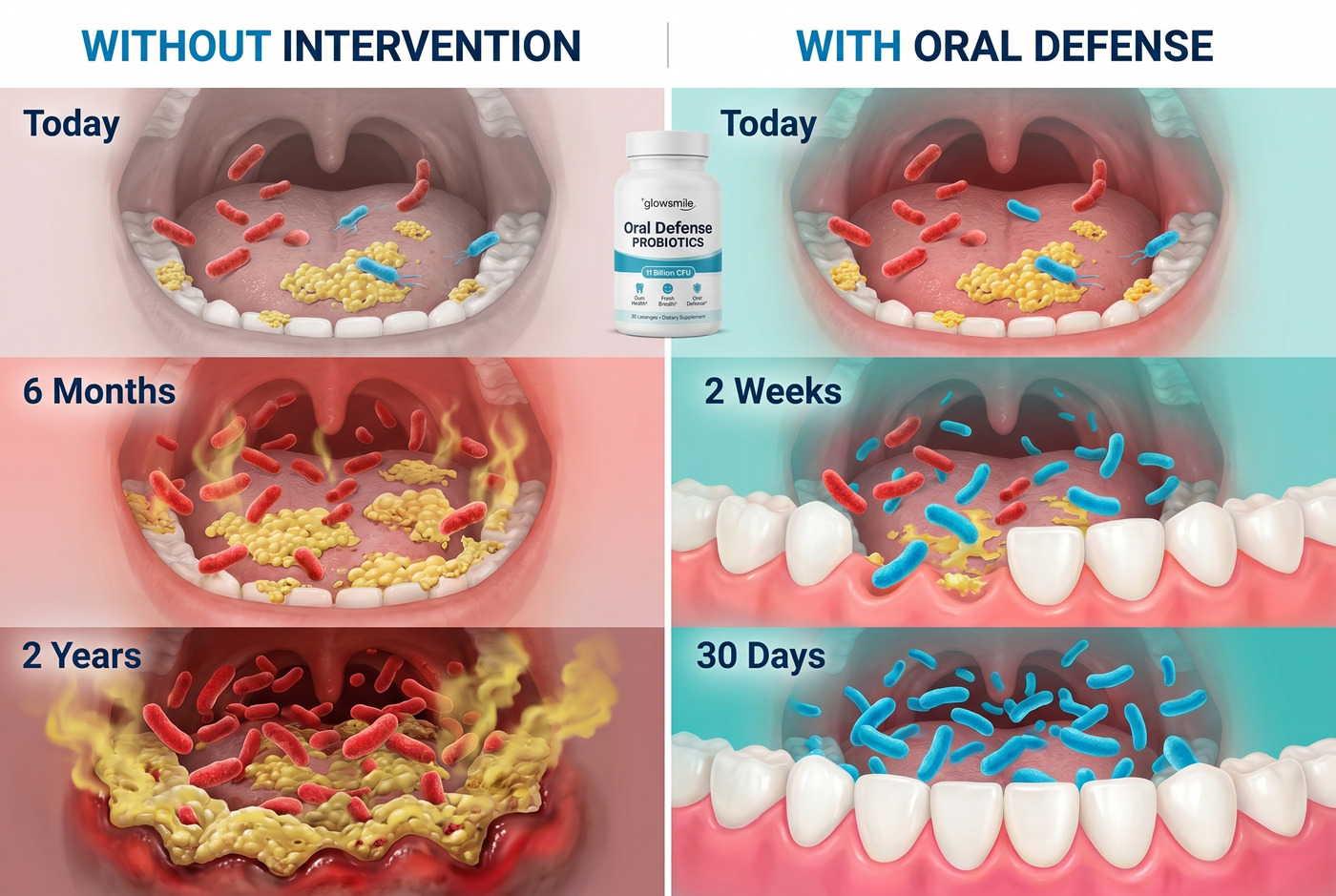
After reviewing the options available, I recommend Oral Defense Probiotics.
Here's why it meets the clinical criteria:
- 11 billion CFU per lozenge — Exceeds the dosing threshold used in published trials
- Contains the exact strains from the research — BLIS K12, BLIS M18, and L. reuteri
- 7 clinically studied strains total — Including supporting strains for complete microbiome restoration
- Lozenge format — Dissolves on the tongue for direct oral cavity colonization
- Third-party strain viability testing — Verifies the probiotics are alive when they reach your mouth
I have no financial relationship with the company. I recommend it because it's the only product I've found that matches the clinical protocol requirements.
Note: This is a dietary supplement. Do not replace prescribed cardiovascular medications without consulting your physician. If you're on blood thinners or have active cardiac disease, discuss this with your cardiologist before starting.
If You Have Chronic Bad Breath AND Any Of These, Pay Attention
Based on my clinical experience and the research:
- Elevated hs-CRP or other inflammatory markers
- Family history of heart disease
- High blood pressure
- Elevated cholesterol
- Type 2 diabetes or pre-diabetes
- Age over 50
- Long-term daily mouthwash use
The combination of chronic bad breath and any of these factors suggests your oral microbiome may be contributing to your cardiovascular risk.
This doesn't mean you're going to have a heart attack. It means you have an inflammatory process happening that has been quietly ignored by both your dental and medical providers.
The research is clear. The intervention is simple. The downside is essentially zero.
Your Oral Microbiome Is Deteriorating Every Month You Wait
Pathogenic bacteria don't stay static.
They multiply. They spread. They build thicker biofilm. They colonize more surfaces. They translocate more bacterial load into your bloodstream.
Every month of continued alcohol mouthwash use pushes your microbiome further toward pathogen dominance. Every year of continued bacterial translocation drives more systemic inflammation. Every decade of this process contributes to the vascular changes I see on imaging.
The men and women I meet in my cath lab — the ones getting stents, bypasses, emergency cardiac intervention — often have histories that include 20 or 30 years of ignored chronic bad breath.
By the time I see them, the damage is cumulative and partially permanent.
You have the ability, right now, to address one of the inflammatory drivers that contributes to cardiovascular disease. It costs about $22 per month. It takes 30 seconds at bedtime.
Or you can keep using mouthwash that's making the problem worse. And find out what your hs-CRP is doing five years from now.
This isn't a category you can substitute. Either you take an oral probiotic designed for the oral microbiome, or you're not treating the cause of chronic bad breath.
WARNING: Oral Defense Probiotics Sells Out Regularly
The company manufactures in limited batches to maintain strain viability.
Every time a story about this research gets shared — including when cardiologists recommend it to their patients — inventory disappears for weeks.
It has sold out 8 times in the past 12 months.
The current stock is already moving.
If you're reading this and it's available, I'd order it today. The next restock after a sellout is typically 3-4 weeks.
APPLY DISCOUNT & CHECK AVAILABILITY

- Limited Time - While Supplies Last
- 30 Day Money Back Guarantee
Limited stock available — Offer ends soon
J
Jack D., 52
Verified Purchase
★★★★★
Finally something that works
I'm 52. My hs-CRP had been climbing for three years and nobody could tell me why. After 90 days on this protocol, it dropped from 4.2 to 1.8. My wife kissed me on the mouth for the first time in years. I didn't even know we'd stopped. My cardiologist saved my life with one recommendation I never expected.
Reviewed on March 15, 2026
47 people found this helpful
M
Margaret D., 63
Verified Purchase
★★★★★
Chronic bad breath
I had chronic bad breath for 20 years. Prescription mouthwashes made it worse. My husband had slept with his back to me since our youngest left for college six years ago. Three weeks after I started this, he rolled over and faced me. I cried into my pillow. Then I asked Dr. Holloway to run my inflammatory markers — they'd dropped 40%. I thought I was buying fresh breath. I bought back my marriage and probably years of my life.
Reviewed on February 8, 2026
20 people found this helpful
IMPORTANT: You Won't Find Oral Defense Probiotics In Drugstores, On Amazon, Or At Big Box Stores

The company sells directly to customers.
No pharmacy markups. No retail distributors inflating the price. No drugstore buyers making decisions about which formulation to stock.
This is why the price stays reasonable — and why the formulation stays at the clinical dose threshold rather than being reduced to hit a big-box retail price point.
The company relies on word of mouth.
Patients share their results because they're stunned by them. And because their cardiologists and primary care physicians aren't telling them.
The fair retail price for a 7-strain oral probiotic of this clinical quality is $97.
Through this link, the introductory price is $54 for a first bottle.
That's less than $2 per day to address one of the silent inflammatory drivers most physicians never think to ask about.
Compare that to:
-
Monthly Listerine + mints + gum: $25-40 (that doesn't work)
-
Prescription antimicrobial rinses: $30-60/month (that makes it worse)
-
ENT specialist consultations: $200-450 per visit
-
The cost of another year of your partner sleeping with their back to you: incalculable
30-Day Money-Back Guarantee
If your breath hasn't significantly improved within 30 days — if you don't notice the changes in your oral microbiome — send it back for a full refund. The company covers return shipping.
Based on the 47 patients I've tracked, I don't expect you'll need to use the guarantee. But it's there.
And here's the thing you'll probably notice first, before anything else:
The person closest to you — who has been silently adjusting around your breath for months or years without telling you — will start leaning in again.
You won't know why they're doing it. They won't know why it changed.
But something will have shifted. Quietly. Permanently.
That's usually the first sign that the work has begun.
Click the button below to secure your offer while it's still available.
APPLY DISCOUNT & CHECK AVAILABILITYUPDATE: As of
The demand has increased dramatically and inventory has been flying off the shelves. Order your own for 50% OFF + FAST SHIPPING before it's too late.
🔥 SELLING OUT!
This is your last chance to get it